Can Continual Pre-training Bridge the Performance Gap between General-purpose and Specialized Language Models in the Medical Domain?
This paper narrows the performance gap between small, specialized models and significantly larger general-purpose models through domain adaptation via continual pre-training and merging.
Can Continual Pre-training Bridge the Performance Gap between General-purpose and Specialized Language Models in the Medical Domain?
The integration of Large Language Models (LLMs) into clinical workflows presents a fundamental tension between transformative potential and operational reality. While general-purpose LLMs excel in standardized benchmarks, the healthcare sector faces two interconnected challenges: the “Language Barrier” and the “Privacy Gap.” Stringent data protection regulations often necessitate on-premise deployments, favoring smaller, computationally efficient models. However, these 7B-class models historically struggle with the nuanced medical terminology and complex reasoning required in specialized fields, particularly in non-English contexts like German.
Our research into the DeFineMed model family addresses a pivotal technical question: Can domain adaptation via continual pre-training (CPT) and sophisticated model merging allow a 7B model to effectively compete with a 24B general-purpose giant?
The DeFineMed Methodology: Building a Specialized Knowledge Base
To overcome the scarcity of high-quality, non-English medical data, we developed the FineMed-de corpus using a hybrid filtering pipeline designed for both precision and scale.
High-Fidelity Data Filtering
We utilized Mixtral-8x7B-Instruct-v0.1 to generate labels for a 260k document subset of the German FineWeb2 split. This pre-classifier achieved an F1 score of 91.1 ± 2.5 against human expert annotators. These labels were used to fine-tune a 279M parameter XLM-RoBERTa classifier. To prioritize data integrity, we implemented a decision threshold of 0.9 and utilized the Fβ score (β = 0.7) as an early stopping criterion, ensuring high precision (0.95) over recall (0.8).
Dataset Comparison: FineMed-de vs. FineWeb2-de
| Dataset | # Documents | # Words |
|---|---|---|
| FineMed-de | 7.3 Million | 5.1 Billion |
| FineWeb2-de | 427.7 Million | 234.8 Billion |
Adaptation and Merge Strategy
The DeFineMed family was adapted from three foundations: Mistral-7B-Instruct-v0.3, Qwen2.5-7B-Instruct, and Mistral-Small-24B-Instruct. Training was conducted on A100 GPUs with limited VRAM (40GB/64GB), necessitating a micro batch size of 1 and the use of Fully Sharded Data Parallelism (FSDP/HSDP). Despite the lower arithmetic intensity, we achieved near-linear scaling using a bin-packing strategy to group sequences into constant-length batches.
To mitigate catastrophic forgetting of instruction-following capabilities, we utilized Spherical Linear Interpolation (SLERP). Unlike uniform merging, we applied a layer-wise, component-specific interpolation schedule, targeting self-attention and MLP layers with gradient schedules to optimize the fusion of domain knowledge and conversational alignment.
The David vs. Goliath Results: 3.5x Performance Gains
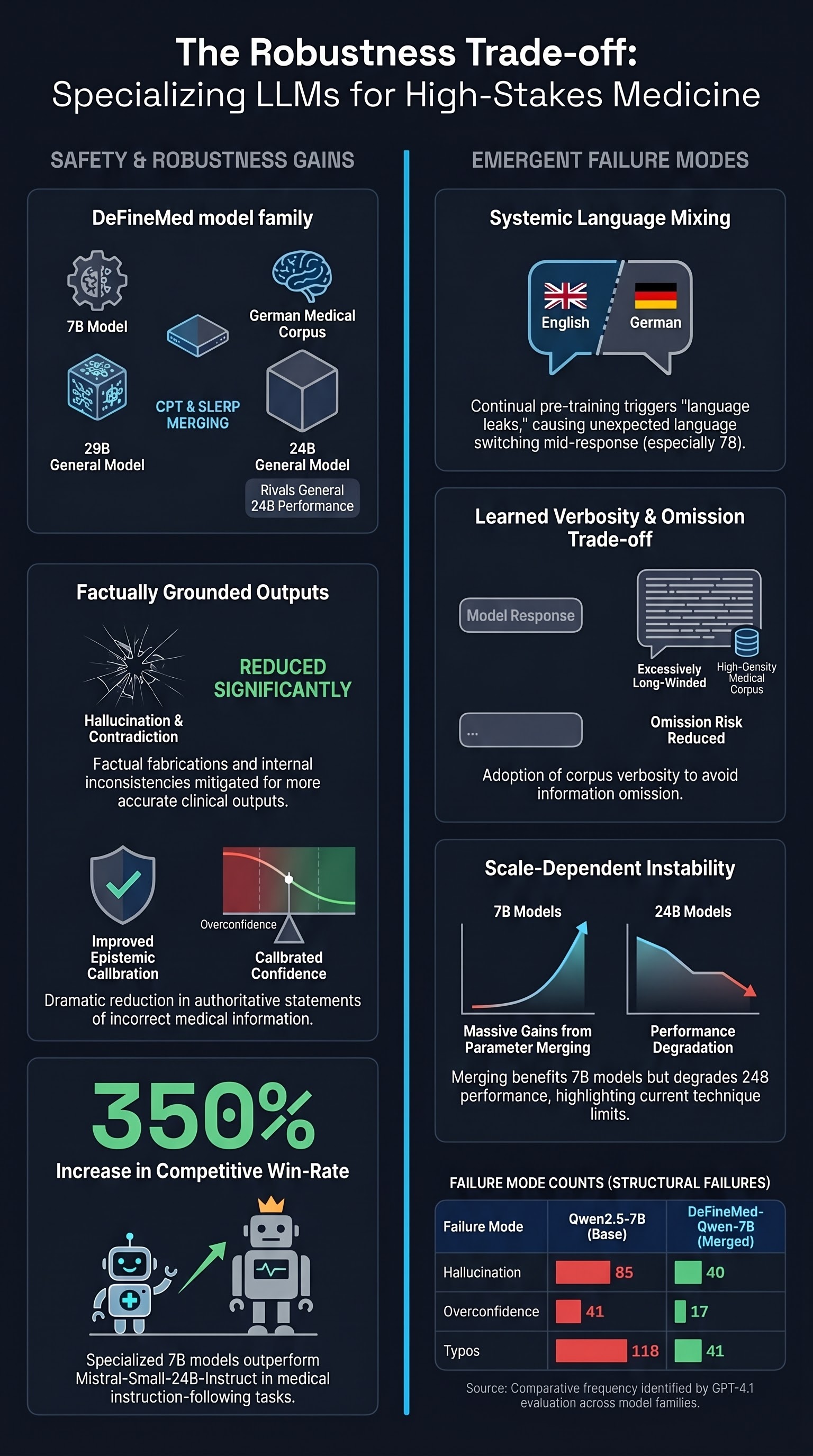
Empirical results demonstrate that domain specialization effectively collapses the performance disparity between model scales. The most significant strategic finding centers on the Qwen2.5-7B-based model. Following domain adaptation, its win-rate against the much larger Mistral-Small-24B-Instruct increased approximately 3.5-fold (climbing from a 0.09 base win-rate to 0.31).
Critical Performance Takeaways
- Closing the Scaling Gap: On German medical benchmarks (MMLU-de and MedQA-de), specialized 7B models drastically reduced the performance delta. The DeFineMed-Qwen2.5-7B-SLERP performed comparably to the non-specialized 24B model in Anatomy and Clinical Knowledge tasks.
- Specialization as a Multiplier: Continual pre-training consistently yielded gains across all architectures. The Mistral-7B variant saw a 6.61% average performance increase across evaluated benchmarks.
- Scale Sensitivity in Merging: While SLERP was essential for instruction recovery, results at the 24B scale were mixed. The Mistral-Small-24B-Instruct base model occasionally outperformed its merged counterpart, suggesting that current merging techniques may degrade performance or hit diminishing returns at larger parameter counts.
Beyond Accuracy: A Failure Mode Analysis for AI Safety
For safety researchers and red-teamers, the objective of domain adaptation extends beyond accuracy to epistemic calibration. Specialization significantly refined how models handle uncertainty and factual grounding, leading to a marked reduction in hallucinations, overconfidence, and contradiction errors.
However, the specialization process introduces systematic failures that distinguish it from purely stochastic errors. Safety practitioners must account for the following trade-offs:
- Language Mixing: The Mistral-7B variant exhibited an extreme failure in language separation. The DeFineMed-Mistral-7B-SLERP showed 207 instances of language mixing out of 216 samples, a massive increase from the 12 instances found in the base model. This indicates that multilingual CPT can severely destabilize a model’s language-routing mechanisms.
- Verbosity and Information Density: Specialized models became significantly more long-winded. This behavior is a direct byproduct of pre-training on a verbose corpus of medical literature, which the subsequent SLERP merge could not fully suppress.
- Low-level Fluency Divergence: We observed contradictory patterns in typo frequency. After specialization, the Qwen2.5-7B family saw typos drop from 118 to 41, while the Mistral-7B family saw an increase from 85 to 125, suggesting that underlying architecture dictates linguistic stability during domain adaptation.
Strategic Takeaways for Practitioners and Researchers
The DeFineMed research provides a blueprint for regulatory-compliant, on-premise AI in healthcare.
- Scale is not the only path to performance. A specialized 7B model can serve as a resource-efficient alternative to general-purpose giants for complex clinical tasks.
- Data quality is the primary engine of specialization. The hybrid filtering pipeline—combining LLM labeling with high-precision classical classifiers—is more critical than raw data volume.
- Merging is a partial fix, not a total solution. While SLERP restores instruction-following, it acts as a “blunt instrument” that can introduce linguistic instability and verbosity.
The future of clinical AI deployment lies in the realization that continual pre-training builds the “brain” (knowledge), but domain-specific instruction tuning provides the “filter” (safety and style). Mitigating the side effects of domain adaptation will require moving beyond simple weight interpolation toward more targeted fine-tuning to ensure both clinical accuracy and behavioral safety.
Read the full paper on arXiv · PDF